What is:
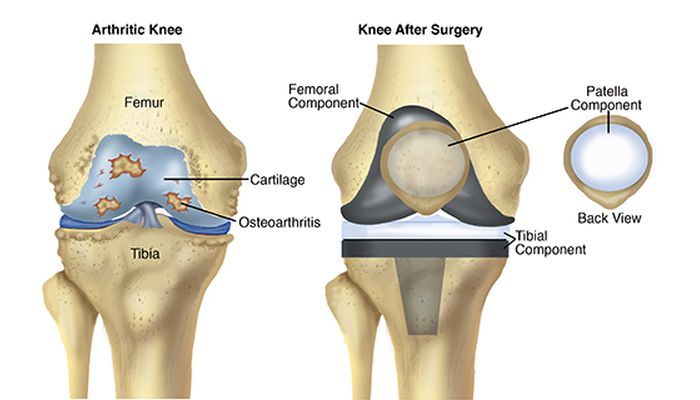
- Arthroplasty / total knee replacement in Delhi is a surgical intervention in which the worn-out joint surfaces of the femur, tibia and often the kneecap are replaced, as they are a source of disabling pain. Metallic and high-density polyethylene components are placed in place of damaged and painful joint surfaces.
Surgery objectives:
- The main objective of placing a total knee prosthesis is to treat the pain caused by arthrosis and, at the same time, to improve joint mobility, increase its functional capacity and return quality of life. In some cases, arthrosis results from a misalignment of the knee in varus or valgus (knees arched or knees together, respectively), and then there is a second objective for knee replacement in Dwarka, which is the correction of this anatomical deformity.
- The joint mobility to be achieved after the surgery will be between 100 to 130 degrees of flexion and the full extension. However, the main factor that determines the postoperative amplitude is the amplitude before surgery, so a knee with reduced mobility will have more difficulty in reaching the intended amplitude.
Indications:
- All patients with an indication for total arthroplasty are frankly limited to activities of daily living, suffering from an intense and disabling painful condition, resistant to medical and physiatric therapy and without any other surgical option. The age factor should be evaluated according to the currently available statistical data, which shows that the survival of total knee replacement in Delhi is 90% at 10 and 80% at 20 years old (defined by the prostheses still functioning) respectively. However, the placement of knee prostheses can be proposed at younger ages, in particular clinical situations that have no other medical or surgical alternative, which will return the patient's quality of life. The majority of patients are in the age group above 60 years, with the upper limit today dependent on general clinical condition, with many cases operated after age 80. The surgical risk will always be assessed in the Preoperative Anesthesiology Consultation. Another important factor, regardless of age, is the motivation of the patient and his family, in the face of disability and suffering caused by arthrosis, after an open discussion of the risks and benefits, especially if there are no serious pathologies, which may condition the patient's longevity.
- The patient with an indication for this surgery has more frequently developed osteoarthritis of idiopathic etiology (a cause is not identified), mechanical due to axis deviation or post-traumatic, due to sequelae of joint fractures.
- Rheumatic diseases, especially rheumatoid arthritis, represent the second most important group of pathologies, due to their joint involvement.
- Excessive body weight is not a contraindication, as long as the patient has a general condition compatible with the surgery. The long-term results are slightly lower, as far as surgery is concerned, however, it must be considered that obesity associated with limited mobility is itself a vicious cycle, both due to the medical pathologies that it originates and due to the greater body weight gain.
- The longevity of the prosthesis mentioned above, motivates us to try whenever possible a more conservative surgical approach in younger patients, defined by age groups below 60 years of age. This approach consists of arthroscopic gestures, osteotomies for axis correction (“straightening crooked legs”) or even physiotherapy associated with medication and infiltrations in the context of regenerative medicine.
Complications / Risks:
- Performing an arthroplasty implies risks that must be known to the patient. Possible postoperative complications include thromboembolism, which motivates mandatory pharmacological prevention, skin complications, and neurovascular injuries. The infection, often referred to as rejection, has an incidence of less than 1%, but may require new surgery to wash and replace the prosthesis.
- The failure of arthroplasty may be due to aseptic detachment (loose components in the absence of infection, due to sensitivity to polyethylene wear) and premature wear of the material. In these cases, it also involves performing a new surgery for its revision/replacement, states orthopaedic in Dwarka.
Surgical technique:
- The surgical technique we use today is called minimally invasive. It consists in the use of smaller skin incisions, but above all in a lesser aggression of the surrounding soft parts (muscles, synovial membrane, ligaments, vessels, and nerves), explains the orthopaedic in Delhi.
- This approach allows for a less painful postoperative period, less blood loss, less risk of infection and a faster and less painful recovery. Most patients are able, after an initial period with support and load of the operated lower limb, with 2 crutches, to resume a gait without assistants for 1 to 2 months, depending on the condition of the contralateral knee.
- In performing this surgery, general or loco-regional anesthesia can be used, depending on the patient's and anesthetist's decision, during the Anesthesiology Consultation.
- The rehabilitation program starts during hospitalization, about 48 hours after surgery, leaving the patient to walk with the help of 2 crutches and able to go up and downstairs.
Postoperative Care:
- The placement of a knee arthroplasty implies limitations for the practice of sports and should avoid activities with impact. However, walking, golf, gym, swimming, dancing, and cycling are allowed. Patients should promote the longevity of their prosthesis, avoiding overweight, intense physical efforts with impact (running), transporting heavy loads and hyperflexion postures.
- Any infection that occurs, anywhere in the body, must be treated early and effectively, due to the risk of bacteremia (bacteria circulating in the bloodstream) that can contaminate the knee prosthesis from a distance. For the same reason, antibiotic prevention should also be systematically applied to all dental or endoscopic manipulations, using your attending physician whenever necessary, suggests the orthopaedic in Delhi.




No comments:
Post a Comment